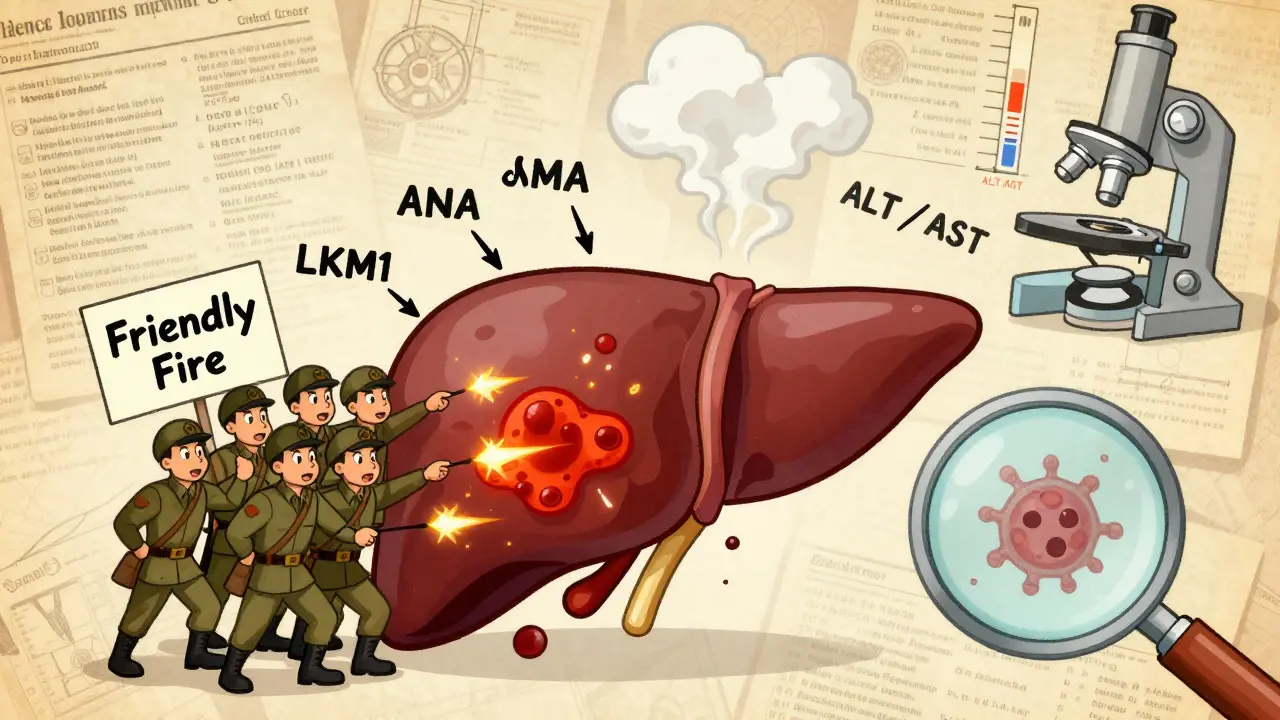
Autoimmune hepatitis isn’t something most people hear about until they or someone they know gets diagnosed. It’s not contagious. It’s not caused by drinking too much alcohol or eating the wrong foods. It’s your own immune system attacking your liver - like a friendly fire incident inside your body. And when it happens, it doesn’t just fade away on its own. Left untreated, it can lead to cirrhosis, liver failure, or even the need for a transplant. The good news? We’ve known how to treat it for decades, and the treatments - steroids and azathioprine - still work better than almost anything else we have today.
How Do You Know You Have Autoimmune Hepatitis?
There’s no single blood test that says, "Yes, you have autoimmune hepatitis." Instead, doctors piece together clues. First, your liver enzymes - ALT and AST - are usually way up. Like, 5 to 10 times higher than normal. That’s a red flag. But so are viral hepatitis, fatty liver, or even a bad reaction to a medication. So the next step is checking for autoantibodies. Most people with autoimmune hepatitis have either antinuclear antibodies (ANA) or smooth muscle antibodies (SMA). A smaller group has LKM1 antibodies. These aren’t just random markers. They’re signs your immune system is targeting liver cells.
But here’s the catch: the type of antibody doesn’t change how you’re treated anymore. The 2025 European Association for the Study of the Liver guidelines dropped the old system of dividing AIH into Type 1 and Type 2 based on antibodies. Why? Because whether you have ANA or LKM1, you still get the same drugs. The focus now is on what’s happening inside the liver.
That’s where the liver biopsy comes in. It’s not fun, but it’s necessary. A needle takes a tiny sample of liver tissue, and under the microscope, doctors look for something called interface hepatitis - inflammation right where the liver’s blood vessels meet the tissue. If you see that, along with high IgG levels (a type of antibody that’s elevated in 80% of cases), and you’ve ruled out other causes like hepatitis B or C, then the diagnosis is solid. The International Autoimmune Hepatitis Group scoring system helps: if your score is over 15, it’s probable. Over 20? Definite.
Why Steroids Are the First Line of Defense
Prednisone (or its cousin prednisolone) has been the go-to drug since the 1970s. It’s not a cure, but it’s a powerful suppressor of the immune system. The goal isn’t to kill the immune system - it’s to quiet it down enough so the liver can heal. Most patients start with 0.5 to 1 mg per kilogram of body weight per day. For a 70 kg person, that’s about 35 to 70 mg daily. That sounds like a lot, and it is. But here’s the thing: most people start feeling better within two weeks. Liver enzymes drop. Fatigue lifts. Some even notice their skin color improves.
But steroids come with a price. Within weeks, side effects show up. Weight gain - especially around the face and belly. Mood swings. Trouble sleeping. Insulin resistance that can lead to diabetes. Bone thinning. Cataracts. About 70% of people on steroid-only therapy deal with at least one major side effect. That’s why doctors don’t keep you on high doses forever. The plan is to taper down. By week 8, you’re usually down to 10-15 mg a day. The goal is to get you as low as possible, as fast as possible - and that’s where azathioprine steps in.
Azathioprine: The Steroid-Sparing Partner
Azathioprine (sold as Azasan or Imuran) isn’t a steroid. It’s an immunosuppressant that works differently. It slows down the immune system by interfering with DNA synthesis in white blood cells. It doesn’t work fast. It takes weeks to months to show its effect. But once it kicks in, it lets you cut back on steroids - often by 70-80%. That’s huge. A 2023 study found that combination therapy (steroids + azathioprine) cut steroid side effects from 70% down to 30%. That’s not just a number - it’s your quality of life.
But azathioprine isn’t risk-free. It can cause nausea, vomiting, or pancreatitis. In rare cases, it can crash your bone marrow, leading to low white blood cells or platelets. That’s why doctors test for TPMT enzyme levels before starting. About 0.3% of people have a genetic variant that makes them unable to break down azathioprine. For them, even a normal dose can be deadly. Testing costs $250-$400, and while it’s routine in Europe, only 45% of U.S. centers do it. If you’re in the U.S., ask for it. It’s not optional - it’s essential.
Most people start azathioprine at 50 mg a day, then increase to 1-2 mg per kg daily (up to 150 mg). It’s usually taken long-term. Some patients stay on it for life. And yes, it’s expensive - branded Imuran can cost $300-$500 a month. But the generic version? $25-$50. Always check for it.
How Long Until You See Results?
It’s not a sprint. It’s a marathon. Most patients show biochemical improvement - meaning ALT and AST levels drop - within 2 to 4 weeks. But true healing? That takes time. The liver needs months to repair the damage. Complete normalization of liver enzymes and IgG levels usually happens between 18 and 24 months. That’s why the 2025 EASL guidelines changed the timeline. Instead of checking response at 6 months, they now recommend waiting 6 to 12 months. Some people just take longer.
By the end of two years, 60-80% of patients reach complete biochemical remission. That means their blood tests look normal. But remission doesn’t always mean the liver is fully healed. That’s why a second biopsy after 2-3 years is often recommended. If the inflammation is gone, you’re in histological remission. That’s the gold standard. And yes - in many cases, the liver fibrosis reverses. One patient on Reddit described going from F3 (advanced scarring) to F0 (no scarring) after two years of treatment. That’s not rare. It’s documented.
What If It Doesn’t Work?
About 10-15% of people don’t respond to steroids and azathioprine. That’s treatment failure. It doesn’t mean you’re out of options. The next step is mycophenolate mofetil (CellCept). It’s taken twice daily, and while it’s pricier - $800-$1,200 a month - it’s effective for many who can’t tolerate azathioprine. Calcineurin inhibitors like tacrolimus are another option, especially for patients with LKM1-positive AIH.
There’s new hope on the horizon. Drugs like tofacitinib (a JAK inhibitor) and clazakizumab (an anti-IL-6 antibody) are in phase 2 trials. Early results show 50-55% response rates in people who failed standard therapy. And obeticholic acid (Ocaliva), originally for primary biliary cholangitis, just got FDA breakthrough designation for AIH. Phase 3 trials showed a 42% complete response rate - better than standard therapy.
Stopping Treatment: The Risky Gamble
Many patients want to stop. Who wouldn’t? Steroids wreck your body. Azathioprine is a daily pill with its own risks. But stopping too soon is dangerous. Studies show 50-90% of patients relapse if they stop treatment. Even if you’ve been in remission for two years, the relapse rate is still 50%. That’s why doctors only consider stopping after 2-3 years of stable remission - and even then, they taper slowly over 6-12 months. And you’re monitored like a hawk. Most relapses happen in the first 3 months after stopping.
Only 45% of attempts to stop treatment succeed. That means more than half need to go back on medication. So don’t rush. Talk to your doctor. If you’re thinking about stopping, get a repeat biopsy. Don’t rely on blood tests alone.
What You Need to Do Before Starting Treatment
Before you take your first pill, there are two critical steps. First, get tested for hepatitis B. About 15-20% of people with AIH have hidden (occult) hepatitis B. If you start immunosuppressants without treating it, the virus can explode. That’s life-threatening. If you’re positive, you’ll need antiviral therapy like tenofovir before starting steroids or azathioprine.
Second, get vaccinated. If you haven’t had hepatitis A or B vaccines, get them now - before you start immunosuppression. Once you’re on steroids or azathioprine, your immune system won’t respond as well. Vaccine effectiveness drops from 90% to 40-60%. Get them early. Protect your liver before you start suppressing your immune system.
Real Stories, Real Side Effects
One patient on Reddit said: "Moon face. 30 pounds of fluid weight in three weeks. Insomnia like permanent jet lag." Another said azathioprine gave them pancreatitis at 100 mg. They switched to mycophenolate - and finally saw their liver enzymes drop.
But there are wins too. A woman in the Autoimmune Hepatitis Association registry said: "After two years on 5 mg prednisone and 75 mg azathioprine, my biopsy showed complete fibrosis reversal." That’s the power of this treatment. It doesn’t just slow things down. It can heal.
Side effects are real. Weight gain. Mood swings. Hair thinning. Fatigue. Bone loss. But they’re manageable. With good monitoring, diet, exercise, calcium and vitamin D supplements, and regular bone density scans, many patients live full lives on these drugs. The alternative - cirrhosis, liver failure - is far worse.
What’s Next for AIH Treatment?
Research is moving fast. The STOP-AIH trial is testing whether people in long-term remission can safely stop treatment. Early data suggests 65% stay in remission - much better than past numbers. The AASLD is developing a patient decision tool to help people understand the trade-offs between side effects and disease control. And biomarkers are being studied. A blood test using microRNA panels can now predict steroid responsiveness within two weeks. That could mean less trial and error.
For now, the standard remains: steroids and azathioprine. It’s not perfect. But it’s effective. It’s been proven. And for most people, it’s life-saving.
Can autoimmune hepatitis be cured?
Autoimmune hepatitis can’t be cured in the traditional sense - meaning, the immune system doesn’t go back to normal. But it can be controlled. With proper treatment, most patients reach remission, where liver enzymes normalize and inflammation stops. Some even see liver scarring reverse. The goal is long-term control, not a cure.
How long do you need to take steroids and azathioprine?
Most patients need treatment for at least 2-3 years. Many require lifelong therapy. About 60-80% of people need maintenance treatment. Stopping too early leads to relapse in 50-90% of cases. If you’re in deep remission for years, your doctor might consider a very slow taper - but only after a repeat biopsy confirms healing.
Is azathioprine safe long-term?
Yes, for most people. The biggest risk is bone marrow suppression, which is rare if you’ve been tested for TPMT enzyme levels. Regular blood tests every 3 months catch any drops in white cells or platelets early. Long-term use is associated with a slightly higher risk of certain cancers, but the risk is low compared to the danger of untreated liver damage.
Why do I need a liver biopsy if my blood tests are normal?
Blood tests show inflammation, but they don’t show healing. A biopsy reveals whether the liver tissue has actually repaired itself. You can have normal ALT levels but still have active inflammation under the surface. That’s why biopsies are used to confirm remission - not just to diagnose.
Can I drink alcohol if I have autoimmune hepatitis?
No. Alcohol adds stress to your liver - and your liver is already under attack from your immune system. Even small amounts can speed up scarring and increase the risk of cirrhosis. Complete abstinence is strongly recommended.
Are there alternatives to steroids and azathioprine?
Yes, but only if you can’t tolerate them. Mycophenolate mofetil is the most common second-line drug. Calcineurin inhibitors like tacrolimus are used for resistant cases. New drugs like JAK inhibitors and monoclonal antibodies are showing promise in trials but aren’t standard yet. For now, steroids and azathioprine remain the most effective and widely used combination.





Jeremy Williams
It’s remarkable how the medical community has refined this treatment paradigm over decades. The shift from antibody-based classification to tissue-level assessment reflects a deeper understanding of disease heterogeneity. I appreciate that the guidelines now prioritize histological remission over biochemical normalization alone. The liver biopsy, while invasive, remains indispensable - it’s the only way to confirm structural recovery. Many patients assume normal ALT means healing, but that’s a dangerous oversimplification.
Also, the emphasis on TPMT testing before azathioprine is critical. In my clinical experience, non-testing centers are essentially gambling with patient safety. A single dose in a TPMT-deficient individual can be fatal. This isn’t optional pharmacology - it’s ethical practice. Why isn’t this mandated nationwide?
And yes, the reversal of fibrosis is real. I’ve seen F3-to-F0 transformations in patients who adhered strictly to treatment and avoided alcohol. It’s not magic. It’s biology.
Maddi Barnes
So let me get this straight 🤔 - we’re giving people high-dose steroids that turn them into Moon Face™ and then slapping on azathioprine like it’s a Band-Aid for a gunshot wound? 😅
And don’t even get me started on the ‘just get vaccinated’ advice… like, sure, doc, I’ll just hop on over to CVS and ask for a Hep B shot while my immune system is still trying to decide if my liver is a snack or a person. 🤷♀️
Also, why is the cost of generic azathioprine $25 but the branded version $500? Is there a secret club where pharmaceutical CEOs vote on how much pain we should feel? 💸
And don’t get me started on the ‘taper slowly’ part. I’ve been on 5mg prednisone for 18 months. My bones feel like they’re made of wet paper. My kids call me ‘Puff’. I’m not ‘in remission’ - I’m in survival mode. 😭
But hey - at least I’m not cirrhotic. So… win? 🤷♀️
Jonathan Rutter
You people are naive. This entire treatment protocol is a scam. Steroids and azathioprine? They’re not treating the disease - they’re treating the symptoms of a system that doesn’t want you to know the real cause.
Did you know glyphosate is linked to autoimmune liver disease? It’s in 90% of processed foods. And the FDA? They’re in bed with Monsanto. The ‘autoimmune’ label is just a distraction so they can sell you drugs instead of fixing the environment.
And why is TPMT testing only done in 45% of U.S. centers? Because the pharmaceutical industry doesn’t want you to know that 0.3% of people are genetically incompatible - because if they did, they’d have to pay for testing. Instead, they bury it in fine print and let people die.
Don’t trust your doctor. Trust your gut. Stop eating bread. Stop drinking water. Go raw. Go alkaline. Go zero-carb. The liver heals itself - if you stop poisoning it with modern medicine.
And don’t even get me started on vaccines. You think they’re protecting you? They’re weakening your immune system so the real villains can take over.
My cousin had AIH. He stopped all meds. Drank lemon water. Did cold showers. Now he’s hiking in Patagonia. No biopsy. No drugs. Just truth.
Jana Eiffel
The evolution of AIH management from serological classification to histological assessment represents a paradigmatic shift toward precision medicine. The abandonment of Type 1/Type 2 dichotomies in the 2025 EASL guidelines is not merely pragmatic - it is epistemologically necessary.
It is striking that the therapeutic response is decoupled from antibody profile, suggesting that downstream inflammatory pathways - rather than upstream autoantigen specificity - are the primary therapeutic targets. This aligns with emerging data on IL-6 and JAK-STAT dysregulation in hepatic stellate cell activation.
Furthermore, the emphasis on histological remission as the gold standard underscores a fundamental truth: biochemical normalization is a surrogate, not a substitute, for tissue repair. Fibrosis reversal, while not universal, is demonstrably achievable - a finding that redefines prognosis.
The ethical imperative to perform TPMT testing before azathioprine initiation is not merely clinical - it is deontological. To withhold it is to violate the principle of non-maleficence.
aine power
Biopsy. Not optional. Period.
Irish Council
Ireland has been doing this right for years. No one here takes steroids without a biopsy. No one. And we test TPMT before the first pill. Why? Because we don’t treat people like lab rats. The NHS does it. Canada does it. The US? You’re playing Russian roulette with a 1 in 300 chance of death. And you wonder why people don’t trust medicine.
Robin bremer
bruh i was on azathioprine for 6 months and i got pancreatitis lmao 😭 my doc just said ‘oh uhh maybe try something else’ and i was like ‘i’m not your guinea pig’ i switched to mycophenolate and now i’m chillin. also steroids made me look like a balloon animal 🤡
Greg Scott
I just want to say - thank you for writing this. I was diagnosed 18 months ago. I was terrified. I didn’t know what to believe. This post gave me clarity. I’ve been on prednisone and azathioprine since day one. My ALT was 1,200. Now it’s 28. I’m not ‘cured’ - but I’m alive. And I’m not going to stop. Not yet.
I’ve gained 40 pounds. I can’t sleep. My bones hurt. But I’m here. And I’m going to keep fighting. For my kids. For my wife. For the next person who Googles ‘autoimmune hepatitis’ and finds this.
Scott Dunne
This is what happens when you let bureaucrats write medical guidelines. You ignore genetics. You ignore environmental triggers. You ignore the fact that glyphosate and EMFs are the real culprits. We’re treating symptoms while the system poisons the source. And you wonder why people get sicker? It’s because you’re not addressing the root - you’re just putting a bandaid on a hemorrhage.
Oana Iordachescu
I’ve been monitoring the literature on AIH for 12 years. The TPMT testing gap in the U.S. is not an oversight - it’s a failure of healthcare infrastructure. We have the tools. We have the data. But we lack the political will to enforce standards. The result? Preventable deaths. And yet, no one is held accountable. The system is broken.
Jayanta Boruah
In India, we rarely use azathioprine due to cost and lack of TPMT testing infrastructure. We rely on mycophenolate from day one. It’s cheaper, safer, and more accessible. The EASL guidelines are Western-centric. Global equity in AIH care requires adaptation - not replication.
Ashley Paashuis
For anyone reading this and feeling overwhelmed - you’re not alone. I’ve been your doctor for five years now. I’ve seen patients go from bedridden to hiking. I’ve seen liver biopsies go from F3 to F0. It’s not easy. But it’s possible.
Take your meds. Avoid alcohol. Get your TPMT tested. Ask for the biopsy. Don’t rush to stop. The goal isn’t to feel ‘normal’ - it’s to live long enough to see your grandchildren.
You’re not a burden. You’re not a failure. You’re a warrior. And your liver is fighting with you.
Michaela Jorstad
I just want to add - if you’re on steroids, please, please, please take calcium and vitamin D. And do weight-bearing exercise. Even walking 20 minutes a day helps. I lost 12% of my bone density in 6 months - and I didn’t know until I had a fracture.
Also - don’t be afraid to ask your doctor for a referral to a dietitian. A low-sodium, high-protein diet makes a huge difference in managing fluid retention and muscle loss.
And if you’re thinking about stopping - please, please, please get a second biopsy. Blood tests lie. Tissue doesn’t.
James Roberts
Okay, I’ll say it - this post is a masterpiece. Clear. Accurate. Human.
And yes - the fact that we still use 1970s drugs as first-line is both terrifying and beautiful. They’re old, but they work. Like a Swiss Army knife in a world of smartphones.
I’m 32. Diagnosed at 28. On 5mg prednisone and 75mg azathioprine. My biopsy last month showed F0. I cried. Not because I’m ‘cured’ - but because I finally feel like I’m not just surviving.
And to the guy who said ‘stop eating bread’ - I’m gonna eat sourdough. And I’m gonna live. Because I’ve earned it.